Have you ever wondered how you see?
I’m naturally curious, so if you’re anything like me, you have probably wondered at some point just how the phenomenon of sight occurs.
(If you’re not, maybe you should start reading now..)
Thankfully, during the course of optometry school, this process was mildly engrained in us, and today, I’m excited to share it with you.
Vision: Explained
First things first: light.
Everything that you see in everyday life corresponds with an electromagnetic frequency within the visible spectrum of light.
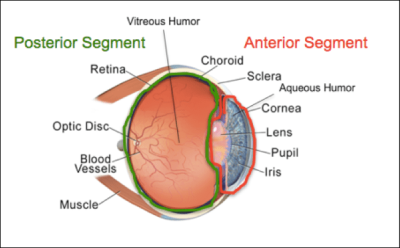
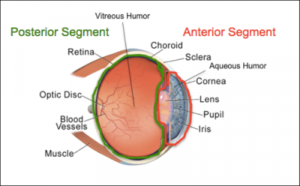
Light enters the eye through the clear cornea, passing through the lens, and ends up at the retina. Together, the cornea and the lens focus the light to attempt to provide a distinct pattern of light on the retina. When they aren’t enough, spectacle or contact lenses are added to help focus the light.
When the light hits the retina, it is sensed by special cells called photoreceptors. The role of photoreceptors is to take the light and transform it into an electrical signal.
Within your eyes, there are different types of photoreceptors: three that require more light to function, and so are utilized in brighter lighting (cones), and one that requires little light to function, allowing it to work in darker conditions (rods). Each of these have specific wavelengths that they are more sensitive to. Three different cells with three different specific wavelengths provides for the perception of color in brighter lighting conditions.
Additionally, cones and rods have specific functions. Cones are responsible for your best vision. For this reason, they are highly concentrated in the most central part of your vision to allow you to see clearly when looking straight ahead. Rods, on the other hand, provide less precise vision, and are located further out from the very central point of vision.
The signal produced by the photoreceptors is then transmitted through additional cells in the retina. These cells help to group, enhance, and refine the signal as it makes its way to the retinal ganglion cells that then pass out of the retina as the optic nerve.
The optic nerve (well, after some minor-ish detours) then passes to the first visual center in the brain – the lateral geniculate nucleus. While it would seem like a primary place for image processing, as this structure is comprised of 6 layers with divided input based on specific types of retinal ganglion cells, relatively little processing occurs here. Rather, it would seem that the lateral geniculate nucleus simply serves to help combine information from both eyes before going further in the brain, or provides an ideal midpoint for information modulation.
From the lateral geniculate nucleus, the signal passes to the primary visual cortex (by way of optic radiations). This is where the first visual processing occurs, allowing for the beginnings of depth perception, a determination of object orientation, and detection of movement.
The signal continues to pass though the other 5 layers of the visual cortex, becoming increasingly refined along the way, until full perception of the image is achieved!
However, simply creating an image does not allow you to react to what you see. Rather, once fully processed in the visual cortex, signals are sent to other areas of the brain (such as Brodmann and Wernicke’s areas) that then give context to the image. Once context is achieved, signals are set to respond appropriately in some form of action – be it smiling at a funny picture, stepping out of the way to avoid someone walking towards you, or reading words off a page!
If you learned something from this post, please share it with a friend or family member! If you liked it, please subscribe, or like my page on Facebook! And as always, if you have any questions or comments, please contact me – I’d love to hear from you!