Happy Friday, y’all!
Guys, like it or not, thanks to COVID-19, it’s the work from home era. If you weren’t using screens most of your waking hours before quarantine began, there’s a solid chance that you are now.
And, if you’re like 90% of computer users, it’s probably taken a bit of a toll on you.
Think back: how many times since March have you experienced
- eyestrain
- eye fatigue
- headaches (especially around the eyes)
- dry or watery eyes
- double vision
- blurred vision
after spending time on a screen?
If you’re anything like me, it’s probably a daily occurrence – one that can cut productivity while exacerbating the high stress environment that seems to characterize this unique time.
Have you ever wondered what causes the symptoms associated with Computer Vision Syndrome?
Then you’ve come to the right spot! Let’s get started!
Computer Vision Syndrome: Potential Causes
Binocular Vision Problems
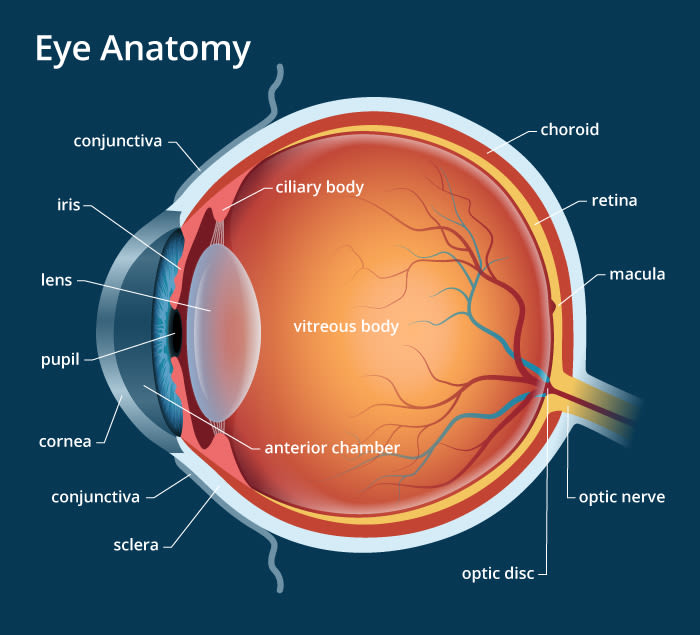
First up: Binocular vision, or the vision that you have when you’re using both eyes.
When you’re using both eyes at the same time, problems generally arise with:
- Vergence – the ability to efficiently turn the eyes in (convergence) or out (divergence)
- Accommodation – the ability to focus (and relax focus of) the eyes
or a combination of the two.
Problems with vergence and accommodation may manifest as:
- eyestrain
- eye fatigue
- headaches
- blurred/double vision
Binocular vision problems may be exacerbated by increased screen-time for several reasons. First, the location of the screen forces the eyes to turn in, or converge. This may cause symptoms in both those who struggle to turn their eyes in (convergence insufficiency) or those who struggle to turn their eyes out (convergence excess).
The close proximity of the screen also forces the eyes to accommodate or focus, to keep the words in focus. Just like with vergence, people may have difficulty bringing the target into focus in the first place (accommodative insufficiency), or relaxing their eyes to refocus at distance (accommodative excess).
Dry Eye
Did you know that the average individual blinks somewhere around 20 times per minute?
This natural phenomenon serves a multitude of functions, from promoting clear vision, to clearing debris, to protecting the ocular surface from irritants, to maintaining the proper moisture for optimal corneal health.
Now, take a guess at how computer use changes blink rate.
- 15 times per minute?
- 10 times per minute?
- 5 times per minute?
The specific numbers vary by report, but in the two studies that I looked at for this discussion, average blink rate was reported to decrease to between 4 and 7 times per minute during computer use.
It’s no wonder that so many people report dry, watery eyes, or blurred vision that momentarily improves with blinking in conjunction with increased screen time!
Blue Light
Yesterday’s discussion, Blue Light: The Conversation Begins, introduced the basics of blue light, and the initial concerns with blue light and ocular health. While these concerns were largely determined to be unfounded, blue light has still been thought to be associated with Computer Vision Syndrome. Since I’m doing a series specifically on blue light, I’ll plan on addressing its potential role in Computer Vision Syndrome in a separate, but related post in the near future, along with another post discussing common treatments for Computer Vision Syndrome. Stay tuned!
If you have any questions or comments, please contact me! If you’ve enjoyed this article, please subscribe, or like my page on Facebook!